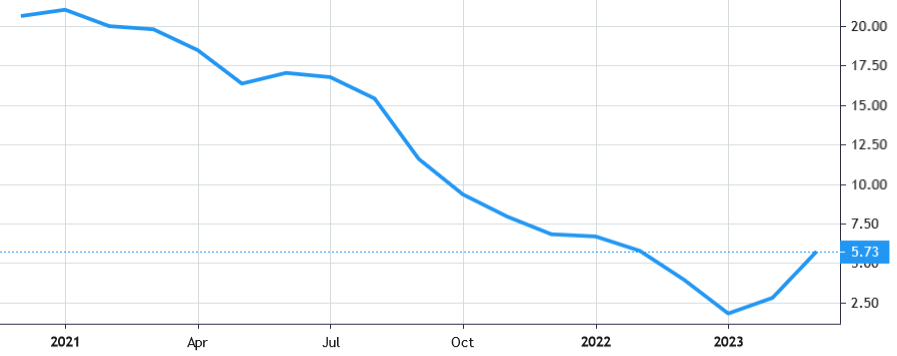
 Stock Value
Stock Value
About Inozyme Pharma
Inozyme Pharma, Inc. operates as a clinical-stage rare disease biopharmaceutical company developing novel therapeutics for the treatment of diseases impacting the vasculature, soft tissue and skeleton. Through its in-depth understanding of a key biological pathway, the company is pursuing the development of therapeutics to address the underlying causes of these debilitating diseases. It is well established that two genes, ENPP1 and ABCC6, play key roles in this critical pathway and that defects in these genes lead to low levels of plasma pyrophosphate, or PPi, which drives pathologic mineralization, and low levels of adenosine, which drives intimal proliferation. The company initially focused on developing a novel therapy to treat the rare genetic diseases of ENPP1 and ABCC6 Deficiencies.
ENPP1 and ABCC6 Deficiencies are chronic, systemic, and progressive diseases occurring over the course of a patient’s lifetime, starting as early as fetal development and spanning into adulthood. These diseases represent a significant unmet medical need, with high mortality rates for infants with ENPP1 Deficiency and high levels of morbidity occurring for patients with these diseases throughout their lives. There are no approved therapies for either ENPP1 Deficiency or ABCC6 Deficiency.
The company’s lead product candidate, INZ-701, is a soluble, recombinant, genetically engineered, fusion protein that is designed to correct a defect in a pathway involving ENPP1 and ABCC6 Deficiencies. This pathway is central to the regulation of calcium deposition throughout the body and is further associated with the inhibition of intimal proliferation, or narrowing and obstruction of blood vessels. The company has generated robust proof of concept data in preclinical models demonstrating that INZ-701 prevented pathological calcification and skeletal abnormalities, led to improvements in overall health and survival and prevented intimal proliferation. INZ-701 is designed to increase circulating levels of plasma pyrophosphate, or PPi, and adenosine. In its preclinical studies conducted in Enpp1-deficient mouse models, dosing with INZ-701 resulted in increased plasma PPi levels, prevention of calcification in the heart, aorta, kidney, liver, spleen and lung, prevention of skeletal abnormalities and improvements in overall health. In Abcc6-deficient mouse models, dosing with INZ-701 also increased plasma PPi levels and prevented calcification in key tissues. In addition to increasing levels of PPi, in preclinical studies, INZ-701 prevented intimal proliferation in both wild-type and Enpp1-deficient mice, which is attributable to increased levels of adenosine.
The company is conducting Phase 1/2 clinical trials of INZ-701 for the treatment of ENPP1 Deficiency and ABCC6 Deficiency. The U.S. Food and Drug Administration, or FDA, and the European Medicines Agency, or EMA, have granted orphan drug designation to INZ-701 for the treatment of ENPP1 Deficiency and ABCC6 Deficiency. The FDA has also granted fast track designation for INZ-701 for the treatment of ENPP1 Deficiency, and rare pediatric disease designation for INZ-701 for the treatment of ENPP1 Deficiency.
In November 2021, the company initiated its Phase 1/2 clinical trial of INZ-701 in ENPP1 Deficiency. The clinical trial initially enrolled nine adult patients with ENPP1 Deficiency at sites in North America and Europe. The trial will primarily assess the safety and tolerability of INZ-701 in adult patients with ENPP1 Deficiency, as well as characterize the pharmacokinetic and pharmacodynamic profile of INZ-701, including evaluation of PPi and other biomarker levels. In the Phase 1 dose-escalation portion of the trial, the company assessed INZ-701 for 32-days at doses of 0.2 mg/kg, 0.6 mg/kg, and 1.8 mg/kg administered via subcutaneous injection, with three patients per dose cohort. Patients received a single dose and then began twice weekly dosing one week later. The Phase 1 dose-escalation portion of the trial is complete. The Phase 2 portion of the trial is ongoing.
In February 2023, the company reported topline data from this trial. INZ-701 activity in a dose proportional manner was observed and a long half-life of approximately 126 hours and drug accumulation as shown by a greater than dose proportional exposure suggests the potential for once weekly dosing. INZ-701 was generally well-tolerated and exhibited a favorable safety profile, with no serious or severe adverse events attributed to INZ-701 and no adverse events leading to study withdrawal. The company plans to report interim clinical data from the ongoing Phase 1/2 clinical trial of INZ-701 in adults with ENPP1 Deficiency in the third quarter of 2023. The company also plans to investigate the potential for once weekly dosing in the ongoing trial.
The company initiated pivotal trial meetings with the FDA in the first quarter of 2023. The company plans to initiate a Phase 1b clinical trial of INZ-701, or the ENERGY-1 trial, to evaluate the safety, tolerability, pharmacokinetics, and pharmacodynamics of INZ-701 in infants with ENPP1 Deficiency in the second quarter of 2023. The company is also actively designing a pivotal trial of INZ-701 in pediatric patients with ENPP1 Deficiency and plans to initiate this trial in the third quarter of 2023, subject to receipt of regulatory approval. The company anticipates initiating protocol assistance meetings with the EMA in the fourth quarter of 2023.
In February 2023, the company dosed its first pediatric patient with ENPP1 Deficiency with INZ-701 under its expanded access program.
In April 2022, the company initiated its Phase 1/2 clinical trial of INZ-701 in adult patients with ABCC6 Deficiency. The trial initially enrolled nine patients with ABCC6 Deficiency at sites in the United States and Europe. The trial will primarily assess the safety and tolerability of INZ-701 in adult patients with ABCC6 Deficiency, as well as characterize the pharmacokinetic and pharmacodynamic profile of INZ-701, including the evaluation of levels of plasma PPi and other biomarkers. In the Phase 1 dose-escalation portion of the clinical trial, the company assessed INZ-701 for 32-days at doses of 0.2 mg/kg, 0.6 mg/kg, and 1.8 mg/kg administered via subcutaneous injection, with three patients per dose cohort. Patients received a single dose and then began twice weekly dosing one week later. The Phase 1 dose-escalation portion of the trial is complete. The Phase 2 portion of the trial is ongoing.
In February 2023, the company reported topline data from this trial. A rapid, significant, and sustained increase in PPi was observed in all cohorts with a dose response observed. PPi showed sustained increase in the highest dose cohort to levels comparable to those observed in its study of healthy subjects (n=10), which study showed PPi levels between 1002 nM and 2169 nM. INZ-701 activity in a greater than dose proportional manner was observed and drug accumulation as shown by a greater than dose proportional exposure suggests the potential for once weekly dosing. INZ-701 was generally well-tolerated and exhibited a favorable safety profile, with no serious or severe adverse events attributed to INZ-701. Seven of the nine patients experienced adverse events related to INZ-701. All adverse events were mild to moderate in severity. One patient from the highest dose cohort (1.8 mg/kg) was withdrawn from the Phase 1 portion of the trial at day 18 due to a moderate adverse event (erythema/urticaria) related to INZ-701. A replacement patient was enrolled in the Phase 1 portion of trial and all nine patients continue in the Phase 2 portion of the trial.
The company plans to report interim clinical data from the ongoing Phase 1/2 trial in adults in the fourth quarter of 2023. Subject to regulatory approval and sufficient funding, it plans to initiate a Phase 2/3 clinical trial in patients with ABCC6 Deficiency in 2024.
Subject to successfully completing clinical development of INZ-701 in ENPP1 and ABCC6 Deficiencies, the company plans to seek marketing approvals for INZ-701 on a worldwide basis. Beyond its development focus on INZ-701, the company’s therapeutic approach has the potential to benefit patients suffering from additional diseases of pathologic mineralization and intimal proliferation, including those without a clear genetic basis, such as calciphylaxis or calcifications as a result of end stage kidney disease, or ESKD. In December 2022, the FDA allowed the company’s IND to enable it to evaluate INZ-701 in a clinical trial in patients with ESKD and calciphylaxis. The company plans to initiate a clinical trial in ESKD patients and it expects data from this trial to inform its development plans in calciphylaxis. The company is also exploring the potential for the development of a gene therapy for ENPP1 Deficiency.
The company retains worldwide, exclusive development and commercialization rights to its pipeline and programs, including INZ-701. The company’s development programs are protected through exclusive intellectual property rights, including with filed and issued patents covering composition of matter for ENPP1-Fc fusion proteins, including INZ-701, and methods of treatment. The company obtained an exclusive, worldwide license to its foundational intellectual property rights from Yale University, or Yale, in January 2017. In July 2020, the company entered into an intellectual property asset purchase agreement with Alexion Pharmaceuticals, Inc., or Alexion, pursuant to which Alexion sold and assigned to it its right, title and interest in and to specified patent rights and other specified assets solely related to ENPP1.
The company has assembled a leadership team with a strong track record and experience in building and managing biopharmaceutical companies and in rare disease research, development and commercialization. The company’s executives have experience, in particular, in developing new markets, obtaining marketing approval for and commercializing therapies for rare diseases that had not previously been the focus for drug development.
The company conducted what is the largest retrospective, cross-sectional, natural history study of infants, children and adults who had GACI or any presentation of ENPP1 Deficiency, including subjects with the acute form of ABCC6 Deficiency who were diagnosed with GACI as infants. The U.S. National Institutes of Health, or NIH, and the University of Münster in Germany contributed data on 127 subjects across 18 countries to this natural history study. Preliminary results from the study suggest that ENPP1 Deficiency, regardless of its phenotypic manifestation or original diagnosis as GACI or ARHR2, appears to be a chronic, systemic, and progressive disease that occurs over the course of a patient’s lifetime.
In 2022, the company initiated a retrospective, longitudinal natural history study of patients with ENPP1 Deficiency and ABCC6 Deficiency and a prospective, longitudinal natural history study of patients with ENPP1 Deficiency and ABCC6 Deficiency.
ENPP1 Deficiency is estimated to occur in approximately one in 64,000 pregnancies worldwide. In North America, Europe and Japan, there are approximately 7,800 patients with ENPP1 Deficiency. In 2022, an analysis of all published cases of ENPP1 Deficiency patients diagnosed with GACI or ARHR2, and two published natural history studies, reported a threefold increase in pathogenic/likely pathogenic ENPP1 variants compared to those identified as of 2020.
ABCC6 Deficiency is a rare, inherited, genetic inborn error of metabolism caused by inactivating mutations in the ABCC6 gene. The systemic and progressively debilitating condition is inherited as a recessive trait in which mutations in the ABCC6 gene result in decreased or absent activity of the ABCC6 protein.
INZ-701 is a soluble, recombinant protein containing the extracellular domain of native human ENPP1 fused to the fragment crystallizable, or Fc, domain of the immunoglobulin IgG1. In its native form, ENPP1 is a transmembrane enzyme with a modular structure consisting of a short intracellular domain, a single transmembrane domain and an extracellular domain that contains a conserved catalytic site responsible for enzymatic activity. ENPP1 is expressed predominantly in the liver and, to a lesser extent, in the kidney and bone. INZ-701 contains the extracellular soluble domain of ENPP1 fused to the Fc domain of IgG1 to minimize immunogenicity, stabilize the construct, increase the plasma half-life and allow ease of purification.
INZ-701 is designed to replace the lost enzymatic function of genetically deficient ENPP1, thus increasing PPi and adenosine, for ENPP1 Deficiency and providing therapeutic effect to treat other diseases, like ABCC6 Deficiency, involving low PPi levels. In contrast to native ENPP1, INZ-701 is a soluble protein that is designed to circulate throughout the body and access extracellular ATP and other nucleotide proteins. Like native ENPP1, INZ-701 cleaves ATP into PPi and AMP, a precursor of adenosine. Pharmacologically, INZ-701 is designed to have prolonged distribution and elimination phases, leading to steady-state concentrations in the blood over time and making dosing possible at infrequent intervals, potentially once-weekly dosing. INZ-701 is formulated for subcutaneous delivery.
In its preclinical studies conducted in Enpp1-deficient mouse models, dosing with INZ-701 resulted in increased plasma PPi levels, prevention of ectopic calcium deposits in a variety of tissues, prevention of calcification in the heart, aorta, lung, kidney, liver and spleen, prevention of skeletal abnormalities and improvements in overall health. In Abcc6-deficient mouse models, dosing with INZ-701 also increased plasma PPi levels and reduced calcification in key tissues. In addition to increasing levels of PPi, in preclinical studies, INZ-701 prevented intimal proliferation in both wild-type and Enpp1-deficient mice, which it is attributable to increased levels of adenosine. The nonclinical INZ-701 toxicology studies that it conducted in two animal species showed no systemic adverse effects at doses that significantly exceeded potential human doses.
The company demonstrated preclinical proof of concept for INZ-701 using multiple mouse models containing inactivated genes for ENPP1. In these Enpp1-deficient mouse models, the animals have an increased propensity for vascular calcification and replicate key aspects of human disease due to ENPP1 Deficiency.
In its preclinical studies, the company also used an ABCC6 mouse model with targeted ablation of the ABCC6 gene. In these mice, ectopic calcification in tissues resembles that seen in human disease due to ABCC6 Deficiency. ABCC6 is primarily expressed in the liver. In mice, ABCC6 is responsible for approximately 90% of the levels of extracellular ATP, the primary source of extracellular PPi. Mice in which the gene for ABCC6 has been inactivated exhibit significantly reduced levels of extracellular PPi in blood.
The company obtained evidence of changes in vascular calcification in asj mice on the acceleration diet by carrying out scans of the heart and aorta using a technique known as high resolution micro computed tomography, or micro CT. All nine asj mice dosed with vehicle control showed variable but extensive calcification in the aorta, coronary artery and heart. All nine asj mice dosed with 0.2 mg/kg of INZ-701 showed a pattern and intensity of calcification signals similar to that shown when mice were dosed with vehicle control. In almost all cases, increasing the dose of INZ-701 to 1 mg/kg or 5 mg/kg completely prevented calcification in the heart and in the aorta.
In another experiment, the company treated mice with either 1 mg/kg of mENPP1-Fc, a research version of INZ-701 containing a mouse Fc domain, or vehicle control starting on the fourteenth day of life and until day 55. In this experiment, all eight mice treated with mENPP1-Fc survived the full 55 days of the trial (represented by the blue line in the graph below), while the median lifespan of the untreated mice decreased from 58 days to 35 days (represented by the black hatched line in the graph below).
In another experiment, the company treated asj mice with 0.2 mg/kg, 1 mg/kg or 5 mg/kg of INZ-701 and vehicle control for 56 days to analyze by micro CT the femora and tibiae bones and measure both trabecular number and cortical thickness, which are two important contributors of bone strength.
The company evaluated INZ-701 in toxicology studies in rats, mice, and non-human primates. In single and multiple administration studies in rats and non-human primates, the maximum tolerated doses of INZ-701 were determined to be 180 and 100 mg/kg, respectively.
Overall, in the company’s nonclinical toxicology studies, INZ-701 exhibited a good safety profile and an acceptable therapeutic index.
In November 2021, the company initiated its Phase 1/2 clinical trial of INZ-701 in adult patients with ENPP1 Deficiency. The Phase 1/2 clinical trial of INZ-701 is an open-label, first-in-human, multiple ascending dose trial, which initially enrolled nine adult patients at sites in North America and Europe. The trial will primarily assess the safety and tolerability of INZ-701 in adult patients with ENPP1 Deficiency, as well as characterize the pharmacokinetic and pharmacodynamic profile of INZ-701, including evaluation of PPi and other biomarker levels. In the Phase 1 dose-escalation portion of the trial, the company assessed INZ-701 for 32 days at doses of 0.2 mg/kg, 0.6 mg/kg, and 1.8 mg/kg administered via subcutaneous injection, with three patients per dose cohort, which doses were selected based on preclinical studies and pharmacokinetic/pharmacodynamic modeling. Patients received a single dose and then began twice weekly dosing one week later.
In April 2022, the company announced preliminary biomarker, safety and pharmacokinetic data from the 0.2 mg/kg cohort of the Phase 1 dose escalation portion of this trial. At the 0.2 mg/kg dose level of INZ-701, all three patients showed rapid, significant, and sustained increases in PPi levels. Preclinical findings demonstrated PPi being a key predictive biomarker of therapeutic benefit in ENPP1 Deficiency.
In November 2022, the company announced the first self-administration of INZ-701 in the open-label Phase 2 portion of the trial.
In February 2023, the company reported topline pharmacokinetic, pharmacodynamic and safety data from this trial. A rapid, significant, and sustained increase in PPi was observed in all dose cohorts and in all patients, with a target PPi threshold observed from the lowest does of 0.2 mg/kg. PPi increased in all patients to levels comparable to those observed in its study of healthy subjects (n=10), which study showed PPi levels between 1002 nM and 2169 nM. The mean baseline PPi across all three cohorts in the trial was 426±407 nM.
INZ-701 activity in a dose proportional manner was observed and a long half-life of approximately 126 hours and drug accumulation as shown by a greater than dose proportional exposure suggests the potential for once weekly dosing. INZ-701 exhibited a favorable immunogenicity profile with low titers of non-neutralizing anti-drug antibodies observed in seven of nine patients. INZ-701 was generally well-tolerated and exhibited a favorable safety profile, with no serious or severe adverse events attributed to INZ-701 and no adverse events leading to study withdrawal. Three of the nine patients experienced mild adverse events related to INZ-701 (including injection site reactions (bruising or pain) occurring in two of nine patients and other mild adverse events included decreased appetite and fatigue). There were two serious adverse events not related to INZ-701. All nine patients enrolled in the Phase 2 portion of the trial, one of whom subsequently withdrew from the study following week 12 due to travel reasons. Eight patients continue in the ongoing Phase 2 portion of the trial on INZ-701 treatment.
The company plans to report interim clinical data from the ongoing Phase 1/2 clinical trial of INZ-701 in adults with ENPP1 Deficiency in the third quarter of 2023. The company also plans to investigate the potential for once weekly dosing in the ongoing trial.
The company also plans to initiate a Phase 1b clinical trial of INZ-701, or the ENERGY-1 trial, to evaluate the safety, tolerability, pharmacokinetics, and pharmacodynamics of INZ-701 in infants with ENPP1 Deficiency in the second quarter of 2023. This single arm, open label, multicenter trial will enroll up to eight patients over a treatment period of 52-weeks. Additional objectives of the ENERGY-1 trial include increasing levels of plasma PPi and assessing the impact of INZ-701 on patient survival, growth, development, functional performance, cardiac function, biomarkers related to bone and mineral metabolism, and healthcare utilization.
The company’s clinical strategy is to link the restoration of plasma PPi levels to measures of clinical efficacy in ENPP1 Deficiency and to establish that plasma PPi could be considered a clinically meaningful pharmacodynamic marker in patients with ENPP1 Deficiency. Subject to ongoing discussions with regulatory authorities in the United States, Europe and other jurisdictions the company plans to pursue registration of INZ-701 for ENPP1 Deficiency with plasma PPi as a primary clinical endpoint if supported by appropriate secondary endpoints.
The company initiated pivotal trial meetings with the FDA in the first quarter of 2023. The company is actively designing a pivotal trial of INZ-701 in pediatric patients with ENPP1 Deficiency and plan to initiate this trial in the third quarter of 2023, subject to receipt of regulatory approval. The company anticipates initiating protocol assistance meetings with the EMA in the fourth quarter of 2023.
In April 2022, the company initiated its Phase 1/2 clinical trial of INZ-701 in adult patients with ABCC6 Deficiency. The Phase 1/2 clinical trial of INZ-701 is an open-label multiple ascending dose trial, which initially enrolled nine adult patients at sites in the United States and Europe. The trial will primarily assess the safety and tolerability of INZ-701 in adult patients with ABCC6 Deficiency, as well as characterize the pharmacokinetic and pharmacodynamic profile of INZ-701, including evaluation of plasma PPi and other biomarker levels. In the Phase 1 dose-escalation portion of the trial, it assessed INZ-701 for 32 days at doses of 0.2 mg/kg, 0.6 mg/kg, and 1.8 mg/kg administered via subcutaneous injection, with three patients per dose cohort, which doses were selected based on preclinical studies and pharmacokinetic/pharmacodynamic modeling. Patients received a single dose and then began twice weekly dosing one week later. The Phase 1 dose-escalation portion of the trial seeks to identify a safe and tolerable dose for further development that increases PPi levels for further clinical development. The open-label Phase 2 portion of the trial will assess long-term safety, pharmacokinetics, and pharmacodynamics of continued treatment with INZ-701 for up to 48 weeks, where patients may receive doses of INZ-701 at home depending on site-specific protocols.
In July 2022, the company announced preliminary biomarker, safety and pharmacokinetic data from the 0.2 mg/kg cohort from the Phase 1 dose-escalation portion of this trial. At the 0.2 mg/kg dose level of INZ-701, all three patients showed rapid and significant increases in PPi levels. Preclinical findings demonstrated PPi being a key predictive biomarker of therapeutic benefit in ABCC6 Deficiency. The mean PPi level across the three patients at baseline was 851 nM. At the 0.2 mg/kg dose level of INZ-701, the mean PPi level observed during the 32-day dose evaluation period across the three patients was 1057 nM, which was within the range observed in the company’s study of healthy subjects (n=10), which study showed PPi levels between 1002 nM and 2169 nM. The range of peak PPi levels observed across the three patients in the 32-day dose evaluation period was 2139-4090 nM. Preliminary pharmacokinetic and INZ-701 enzymatic activity remained consistent with data reported from the company’s ongoing Phase 1/2 trial of INZ-701 in patients with ENPP1 Deficiency. INZ-701 continued to exhibit a favorable initial safety profile.
In February 2023, the company reported topline pharmacokinetic, pharmacodynamic and safety data from this trial. A rapid, significant, and sustained increase in PPi was observed in all cohorts with a dose response observed. PPi showed sustained increase in the highest dose cohort to levels comparable to those observed in its study of healthy subjects (n=10), which study showed PPi levels between 1002 nM and 2169 nM. Mean baseline PPi across all three cohorts in the trial was 947±193 nM. PPi levels observed after INZ-701 administration are shown in the table below:
INZ-701 activity in a greater than dose proportional manner was observed and drug accumulation as shown by a greater than dose proportional exposure suggests the potential for once weekly dosing. INZ-701 was generally well-tolerated and exhibited a favorable safety profile, with no serious or severe adverse events attributed to INZ-701. All adverse events were mild to moderate in severity. Seven of the nine patients experienced adverse events related to INZ-701 (including mild injection site reactions (discoloration, erythema, induration, pain or pruritus) occurring in four of the nine patients and other adverse events included erythema, fatigue, night sweats and urticaria).One patient from the highest dose cohort (1.8 mg/kg) was withdrawn from the Phase 1 portion of the trial at day 18 due to a moderate adverse event (erythema/urticaria) related to INZ-701. A replacement patient was enrolled in the Phase 1 portion of trial and all nine patients continue in the Phase 2 portion of the trial.
The company plans to report interim clinical data from the ongoing Phase 1/2 trial in adults in the fourth quarter of 2023.
Subject to regulatory approval and sufficient funding, it plans to initiate a Phase 2/3 clinical trial in patients with ABCC6 Deficiency in 2024.
The company intends to explore the potential of INZ-701 as a therapy in other, non-genetic diseases of pathologic mineralization associated with low levels of PPi, such as calciphylaxis or calcifications as a result of ESKD. Calciphylaxis, a manifestation of CKD, is a non-genetic condition associated with vascular calcification and low PPi levels with a reported one-year survival rate of approximately 50%.
The company has collaborated with a major academic institution to confirm that PPi levels are low in patients with calciphylaxis and to investigate associated manifestations that may be treated with INZ-701. Evidence of low PPi in calciphylaxis is supported by a third-party exploratory study designed to measure PPi in patients with calciphylaxis and to examine whether PPi levels are predictive of clinical outcomes.
The company plans to continue to develop new and innovative therapies to treat ENPP1 and ABCC6 Deficiencies. The company is well-positioned to do so because of its in-depth knowledge of the biological pathways involved in mineralization and of diseases of pathologic mineralization. The company has identified a gene therapy construct having an optimized ENPP1-Fc sequence driven by a tissue specific promoter in its enzyme replacement therapy program that has shown restoration and sustained enzyme activity leading to an increase of plasma PPi levels in preclinical experiments without adverse effects.
In another study in asj/2j mice, the company evaluated lower doses of an AAV vector containing a modified ENPP1-Fc driven by a tissue specific promoter at three different doses by a single intravenous injection for a period of ten weeks. These studies demonstrated increases in plasma PPi with corresponding prevention of calcification in various tissues, including the aorta, spleen and lung, as well as prevention of skeletal abnormalities. such as rickets in the growth plate and ectopic calcification in the vertebrae as shown in the figures below.
Commercialization
The company retains worldwide, exclusive development and commercialization rights to its pipeline and programs, including INZ-701. The company will be able to commercialize INZ-701, if approved, for ENPP1 or ABCC6 Deficiency with a small, targeted, internal sales and commercial organization in the United States and other major markets. The company intends to continue to engage with patient advocacy groups, medical centers of excellence and medical specialists in an effort to expeditiously bring its therapy to patients.
Strategy
The key elements of the company’s strategy are to efficiently advance clinical development for its lead product candidate, INZ-701, with an initial focus on ENPP1 and ABCC6 Deficiencies; expand its research and development efforts for INZ-701 in additional diseases of pathologic mineralization and for other therapies beyond INZ-701; establish commercialization infrastructure for the marketing and sale of INZ-701 for rare indications; build a patient-focused company to treat diseases of pathologic mineralization; and continue to expand its scientific understanding of pathologic mineralization and intimal proliferation, its related intellectual property portfolio and its rights to complementary technologies.
Intellectual Property
Yale University License Agreement
In January 2017, the company entered into a license agreement with Yale, which was amended in May 2020 and July 2020, pursuant to which Yale granted it an exclusive, worldwide license, with specified rights to sublicense, under Yale’s interest in specified intellectual property rights and materials for specified therapeutic and prophylactic products; a nonexclusive, worldwide license under Yale’s interest in the same intellectual property rights and materials for specified diagnostic products; and a nonexclusive, worldwide license under Yale’s interest in specified know-how for specified products, in each case that use any ectonucleotide pyrophosphatase/phosphodiesterase enzymes, or ENPPs, or an agonist or antagonist of ENPP, its receptors, substrates, or ENPP enzymatic products, subject to certain exceptions.
As of March 22, 2023, the company owned or possessed exclusive rights to approximately 22 issued U.S. patents, two pending U.S. provisional patent applications, 18 pending U.S. non-provisional patent applications, 19 issued foreign patents (including three issued European patents), 140 pending foreign patent applications, and three pending Patent Cooperation Treaty applications.
In addition, as of March 22, 2023, the company owned approximately two allowed U.S. trademark applications, two pending foreign trademark applications, and twelve foreign registered trademarks.
INZ-701
The intellectual property portfolio for INZ-701, the company’s most advanced program, as of March 22, 2023, is summarized below. Prosecution is a lengthy process, during which the scope of the claims initially submitted for examination by the U.S. Patent and Trademark Office may be significantly narrowed before issuance, if issued at all.
The company’s patent protection includes patents and patent applications that it has exclusively licensed under its license agreement with Yale. This licensed patent portfolio includes:
A patent family that includes seven issued U.S. patents relating to reducing and/or preventing progression of pathological calcification, reducing or preventing ectopic calcification of soft tissue, reducing or preventing pathological ossification, treating, reversing or preventing progression of ossification of the posterior longitudinal ligament, treating aging-related hardening of arteries, reducing or preventing progression of chronic kidney disease, end-stage renal disease, calcific uremic arteriolopathy, and calciphylaxis, and reducing pathological calcification of vascular tissue in a human subject in need thereof having reduced ENPP1 activity or a loss of function mutation in the gene encoding ENPP1. All such methods of treatment involve administration of soluble ENPP1 that lacks a bone targeting domain. These U.S. patents are expected to expire in 2034, absent any term adjustments or extensions. Corresponding foreign applications have been filed and are pending in Europe, Japan, and Hong Kong, and one patent has been granted in Japan.
A patent family that includes one issued U.S. patent covering certain compositions that contain ENPP1, including INZ-701. This U.S. patent is expected to expire in 2036, absent any term adjustments or extensions. Corresponding foreign applications have been filed and are pending in Europe, Japan, Australia, Canada, Brazil, India, Hong Kong, South Korea, Mexico, New Zealand, and Russia, and one patent has been granted in Australia, Mexico, Russia, and Japan.
Other
Through its acquisition of intellectual property assets from Alexion, the company has acquired, among other assets:
A patent family that includes one issued European patent relating to polypeptides comprising ENPP1 and the therapeutic use of such polypeptides, such as in the treatment of generalized arterial calcification of infancy. This European patent is expected to expire in 2031, absent any term adjustments or extensions.
A patent family that includes two issued U.S. patents relating to compositions and fusion proteins comprising ENPP1 and a targeting moiety. These U.S. patents are expected to expire in 2031, absent any term adjustments or extensions.
A patent family that includes one U.S. reissue patent application relating to methods for treating a subject having PXE by administering to the subject soluble ENPP1.
The term of individual patents depends upon the legal term of the patents in the countries in which they are obtained. In most countries in which the company files, the patent term is 20 years from the earliest date of filing a non-provisional patent application.
In the United States, the term of a patent covering an FDA-approved drug may, in certain cases, be eligible for a patent term extension under the Drug Price Competition and Patent Term Restoration Act of 1984 as compensation for the loss of patent term during the FDA regulatory review process. The period of extension may be up to five years, but cannot extend the remaining term of a patent beyond a total of 14 years from the date of product approval. Only one patent relating to an approved drug may be extended among those patents eligible for an extension and only those claims covering the approved drug, a method for using it, or a method for manufacturing it may be extended. Similar provisions are available in Europe and in certain other jurisdictions to extend the term of a patent that covers an approved drug. It is possible that issued U.S. patents covering the use of INZ-701 and products from its intellectual property may be entitled to patent term extensions.
Research and Development Expense
The company’s research and development expense included $47.8 million for the year ended December 31, 2022.
Government Regulation
In the United States, the company’s product candidates are regulated as biological products, or biologics, under the Public Health Service Act, or PHSA, and the Federal Food, Drug and Cosmetic Act, or FDCA, and its implementing regulations and guidance.
History
Inozyme Pharma, Inc., a Delaware corporation, was founded in 2015. The company was incorporated in 2015.
